
hear.com – India’s leading destination for advanced hearing aids & expert care
Positional vertigo
What you should know
Benign paroxysmal positional vertigo (BPPV) is a feeling of dizziness that occurs depending on a change in position. The reason for this is the detachment of otoliths (ear stones) from the macular organs utriculus and sacculus, which also reach the semicircular canals belonging to the equilibrium organ, which leads to dizziness. Below you will find information on causes, symptoms, and therapy.
Table of Contents
- Positional vertigo symptoms
- Positional vertigo therapy
- Possible complications
- What can cause positional vertigo?
- Other forms of vertigo
Symptoms
The word “benign” is self-explanatory, while “paroxysmal” means attacks. The positional vertigo is considered harmless in principle, but it is extremely uncomfortable for all those affected. It can also be referred to as vertigo, which usually occurs as soon as the head is quickly changed in its position. This vertigo is often referred to as a carousel in the head (carousel vertigo). It can occur in the following situations:
- When turning over in bed
- When getting up from a lying position
- When bending over quickly
- When turning on the affected side
Frequency, age and gender of those affected
Benign positional vertigo affects around 2 in 100 people. Dizziness is more likely to occur in older people. Thus, the condition occurs most frequently between the ages of 50 and 60, while the age peak is between the ages of 60 and 80. Women are affected much more often than men. Regardless of whether the condition has been treated or not, the dizziness recurs in 30-50% of those affected. With special exercises by the ENT doctor, the person affected can also undergo treatment at home on their own.
Positional vertigo exercises

Benign and paroxysmal vertigo cannot be treated with medication, as this would be ineffective according to the current state of knowledge. Instead, treatment takes place using positioning exercises. They serve to guide the detached particles back into the otolith organs – the utricle and sacculus. There are different types or forms of positional vertigo. The most common is the more forward (anterior) and the further back (posterior) forms, whereby the anterior and posterior semicircular canals are meant. Exercise can usually resolve dizziness. Both forms can be treated with the Sémont or the Epley maneuver.
Sémont maneuvers
During this maneuver, the patient sits upright in front of the doctor, and turns their head 45 ° so that the affected side faces the doctor. Then the patient is abruptly shifted sideways on the affected side. Their head remains in the same position. Accordingly, the patient is now lying sideways on the bed, looking “up”. The patient remains in this position for 2-3 minutes, then the patient is repositioned by 180 ° to the other side of the body. The head is held in the same position so that the patient is now looking towards the surface. Then the patient is slowly brought back to the starting position and left there for 3 minutes.
The Sémont maneuver explained in three simple steps:
- Upright sitting position (1)
- Tilt body on shoulder (2)
- Quick turn by 180 ° on the other shoulder; Adjust the maneuver for the right or left ear as required (3)

Epley maneuver
This maneuver was invented by Dr. John Epley in 1980. The patient sits upright with his legs straight in front of the examiner. Their head is turned 45 ° to the affected side, so the examiner is looking at the healthy ear. This is followed by rapid positioning in the supine position, with the head protruding beyond the edge of the examination table (head hanging position). The patient must remain in this position until the vertigo and nystagmus have subsided (at least 1 minute). When the symptoms have subsided, the patient turns his head 90 ° to the healthy side and lingers again until the symptoms have subsided (approx. 1 minute). Then the patient turns on the healthy side, with the head remaining in the position previously assumed, here too it lingers for about 1 minute. The last step in this maneuver is to sit up in the upright position. In order to avoid nausea caused by vertigo attacks during the Epley maneuver as far as possible, the patient should close his eyes.
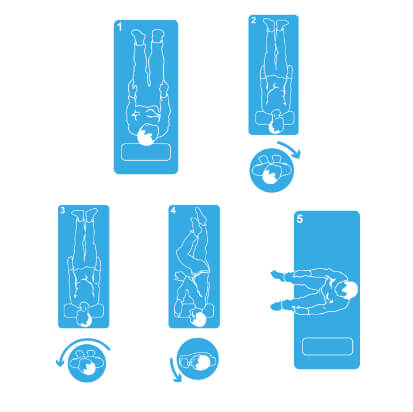
Instructions for the Epley maneuver in 5 steps:
- Upright sitting position, turn head 45° to the right (1)
- Lying position (2)
- Turn head 90° to the left (3)
- Rotate whole body 90° to the left (4)
- Stand up with the head tilted slightly towards the left shoulder; perform the maneuver for the left ear in a mirror-inverted direction (5)
Course and complications
Positional dizziness is an uncomfortable condition, but it is harmless in itself. It often goes away without appropriate therapy, but there are exceptions. Cases are known in which there was a longer course. Dizziness can therefore persist for a period of a few days over several weeks and months up to several years. This is also the reason why an early visit to the ENT doctor is urgently recommended. Even if the form of dizziness often disappears on its own, there is a risk of being confronted with the unpleasant symptoms over a longer period of time.
In the case of benign and paroxysmal positional vertigo, there are usually complications that can make everyday life much more difficult. Especially if the dizziness attacks are not cured by treatment, those affected must learn to deal with the symptoms. This can be very stressful, for example if the patient wakes up from sleep due to dizziness. The condition and the associated imbalance can also increase the risk of falling. If the vertigo persists longer, A person’s general behavior and well-being can also be negatively affected.
Origin and causes
In general, the benign positional vertigo is accompanied by a detachment of the ear stones, which then reach the semicircular canals. This moves them to the new deepest point. The fluid in the semicircular canals starts to move, which leads to a deflection of the cupula (gelatinous cone in the posterior semicircular canal). As a result, the affected semicircular canal is excited. There can be various reasons why the otoliths peel off:
- Inflammation of the organ of equilibrium in the inner ear
- Previous traffic and sports accidents
- Head trauma or injury to the head
- Advanced age
If there are disruptions or a failure of the equilibrium organ, there is a possibility that spatial information is incorrectly passed on to the brain. As a result, typical vertigo can develop. However, the exact cause of the detachment of the otoliths is unknown.
Can there be permanent damage?
Positional vertigo itself is considered harmless, but it is definitely a burden. Dizziness can lead to psychological consequences. In addition, there is a risk of falling due to attacks of vertigo. Accordingly, any work that involves elevated positions or climbing a ladder should be avoided during an existing vertigo.
What is an archway?
A semicircular canal is part of the balance organ in the inner ear. This is a circular tube that is filled with liquid and has tiny hairs on it that are connected to nerve cells. All movements of the body cause the fluid in the semicircular canals and thereby the hairs to move with it. The movement stimulus is passed on to the brain via the nerve cells.
Other forms of vertigo
In addition to positional vertigo, there are other forms of vertigo that have other causes. Meniérè’s disease is caused by pressure in the balance and hearing organs. This is usually accompanied by nausea, sweating, and vomiting. Only one ear is affected, which can develop tinnitus and hearing loss. Strong psychological stress can also trigger vertigo. In cases of brain damage, there is also the possibility that central vertigo is present, which should always be examined by a doctor.
Positional vertigo in the toddler
Positional dizziness is rare in children. Although dizziness and problems with balance are not uncommon in childhood, this is often due to a migraine or other ailments. The detachment of otoconic crystals can already be demonstrated in children, but this does not necessarily cause them to feel dizzy. Medicine does not know exactly why the otoliths loosen. It is assumed that the risk increases with increasing age and thus the likelihood of benign positional vertigo increases from the age of 35.
The history of positional vertigo
The first description of benign positional vertigo goes back to the otologist Róbert Bárány around 1920. In 1969, HF Schuknecht gave the cause research new impetus. While examining deceased patients with positional vertigo, he noticed residues of ear crystals on the cupula. Four years later, the cupulolithiasis theory was replaced by a more conclusive one about the cause of positional vertigo by Schuknecht and Ruby. Nevertheless, the cause is still not fully understood, as no recovery can occur despite ideal treatment.
What is the cupulolithiasis theory?
The theory states that ear crystals are deposited on the cupular organ in the posterior semicircular canal. The otolith forms a preponderance of gravitational forces at this point, which leads to vertigo and the other known symptoms.
What is the Canalolithiasis Hypothesis?
According to this hypothesis, the dizziness is caused by a triggered trauma or by degenerative effects. Small particles of the otoliths become detached and in free movement form a kind of “plug” in the posterior semicircular canal, which leads to an almost complete blockage of the lumen (interior of hollow organs). By quickly positioning the head, the plug can be moved to the opposite side and out of the semicircular canal. This then brings on typical vertigo symptoms.



